Author: admin
stock here: what is amazing is they recommend this for old people. Old people much more likely to have a severe adverse reaction, or death.
This is the video of her collapsing on stage
stock here: I am laying claim to this. As far as I know, I am the first person (outside of the criminals that knew but were keeping it their club secret) that the jabs were all different and that there were killer batches, and also specialty “maiming batches” and this was in July of 2021, at which point I published and then Google methodically wiped me off the map. I was quite sure of my data, but this reaction of being right over the target is what convinced me. Now it is much more mainstream.
 Dear Friends, Dear Friends,This is perhaps one of the most important videos I have shared to date. It reveals even more than we already know and is at the heart of this war we are in both scientifically and existentially. Former Pfizer VP of R&D (who I very much respect), shows scientific data exposing the reason for the large variation and range of Injuries & Deaths from the experimental injections. There is clear evidence that the Batch contents are different! He describes this deliberate difference between the batches as “The Calibration of a Killing Weapon.” He and thousands of other doctors around the world are frantically trying to warn the masses of the devastating effects of the experimental COVID vaccines being mass injected into a largely unsuspecting public, assisted by military forces around the world.  What motivates these doctors, nurses, and scientists to make such an impassioned plea? They have NOTHING TO GAIN, and much to lose, including their careers, and possibly even their lives. What motivates these doctors, nurses, and scientists to make such an impassioned plea? They have NOTHING TO GAIN, and much to lose, including their careers, and possibly even their lives.So why are they doing this? Because they are doctors and scientists who have actually looked behind the smokescreen corporate narrative, and know the devastating potential consequences to those who chose to get this very toxic and dangerous vaccine. They desire to save as many people as possible from the carnage this vaccine is causing, including DEATH, vascular and neurological injuries, life-long autoimmune disease, infertility, and more. Please watch this video, watch to the end, and then share it with as many people as you can, because time is very short! Even if you or someone you love has already taken one or more of the jabs, we are now encouraged to know there are solid ways to mitigate some of the damage, though the harm to your DNA is considered permanent. Praying continually for God’s mercy and grace, ~Jacqueline “Blessed is the man who remains steadfast under trial, for when he has stood the test he will receive the crown of life, which God has promised to those who love him.” ~James 1:12  Heal Infection or Injection: Mercola’s Food List to Clear S Protein Damage Heal Infection or Injection: Mercola’s Food List to Clear S Protein Damage  Dr. Bryan Ardis Gives Life-Saving Protocol & Insight Here Dr. Bryan Ardis Gives Life-Saving Protocol & Insight Here  Ethylene Oxide, FDA PCR Swab Recall, & Strange Black Fibers That Move Ethylene Oxide, FDA PCR Swab Recall, & Strange Black Fibers That Move  Did Gov’t Sway Evangelical Leaders to Promote the Jab to Churches? Deep Roots at Home PO Box 14 Maxwell, IN 46154 You received this email because you signed up on our website to receive one of our seasonal free resources. We hope you’ve enjoyed! If you would prefer to NOT receive emails that cover “warning topics” about current events, medical information, parental rights, and more, PLEASE CLICK HERE to update your subscription preferences. Or you may unsubscribe Did Gov’t Sway Evangelical Leaders to Promote the Jab to Churches? Deep Roots at Home PO Box 14 Maxwell, IN 46154 You received this email because you signed up on our website to receive one of our seasonal free resources. We hope you’ve enjoyed! If you would prefer to NOT receive emails that cover “warning topics” about current events, medical information, parental rights, and more, PLEASE CLICK HERE to update your subscription preferences. Or you may unsubscribe |
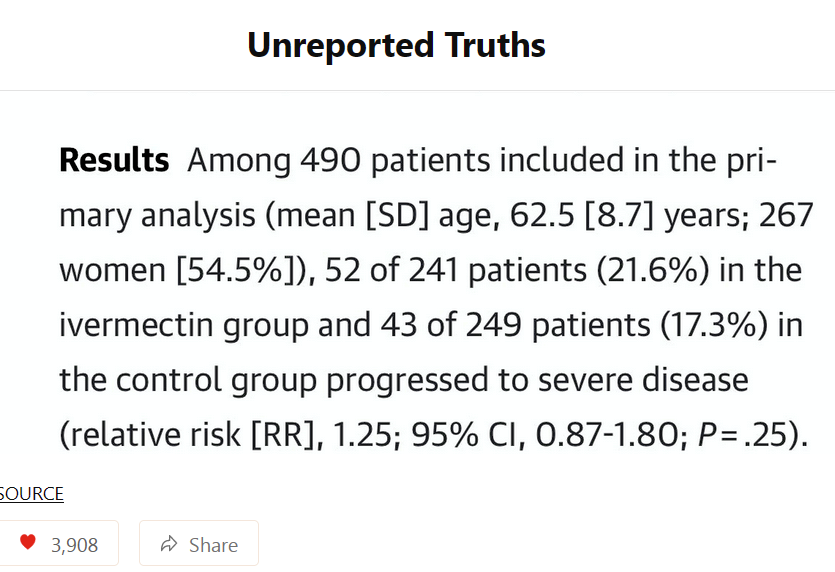
Look at these asshats in the Study, just from reading the first few paragraphs I knew they were targeting against Iver……and then deep in the study—-they have this.
“Patients were encouraged to take Ivermectin with food or after meals to improve drug absorption. ” Which is exactly wrong, taken and hour before food (at least) with a full glass of water.
https://www.mayoclinic.org/drugs-supplements/ivermectin-oral-route/proper-use/drg-20064397
In some categories of analysis, the data did not show a benefit. But the deaths…..10 dead in the control group, only 3 dead in the Ivermectin group. That is so beyond huge!
Did I mention that JAMA was a piece of shit also?
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2789362
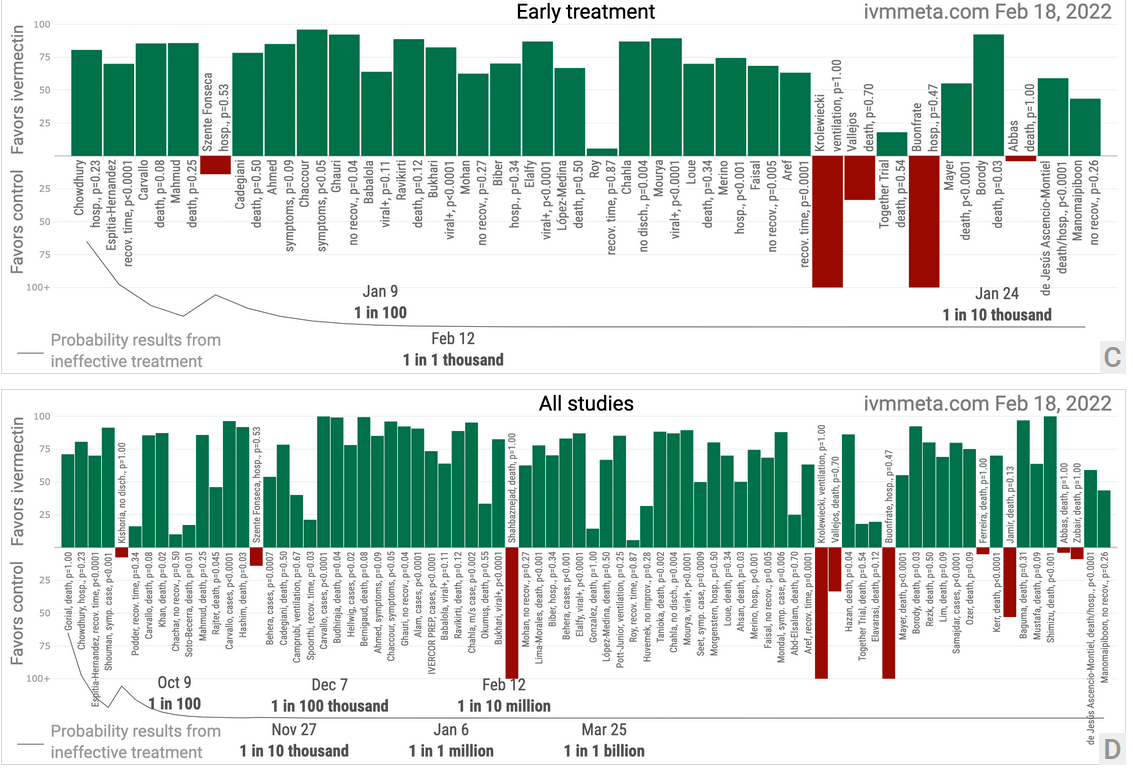
The paper combines a boatload of studies, and summaries using whiskers for uncertainty.
They calculate a less than 1 in 1 billion chance that Ivermectin is actually not beneficial.
stock here: also the media general propaganda is accelerating if that is even possible. And the Russia fear narrative is apparently strong enough that the FDA continues to hold off Jabbing babies with deadly poisons. You know….spread the fear out a bit.
This is from a Twitter Thread Reader App, so I think you don’t need twitter to access this. Nice number 33 articles gathered — damn them to hell.
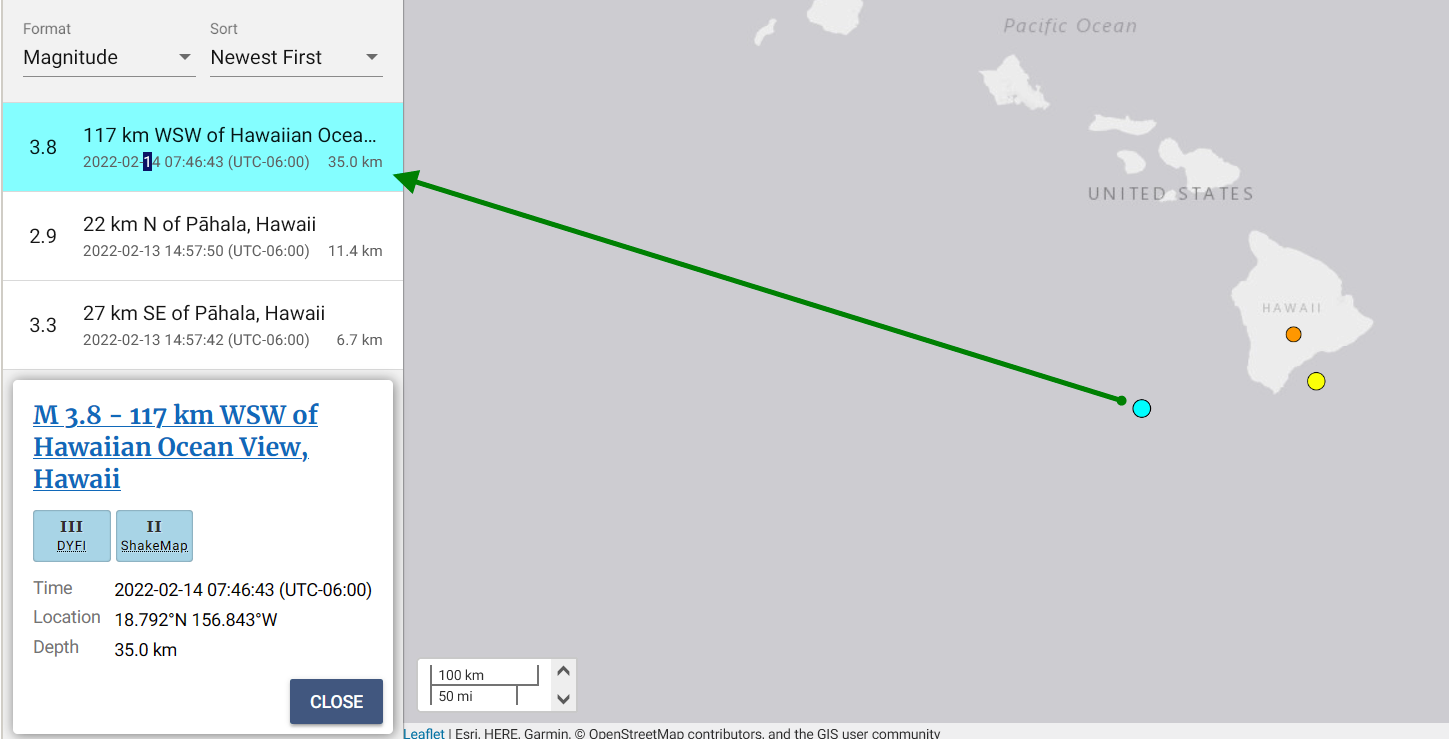
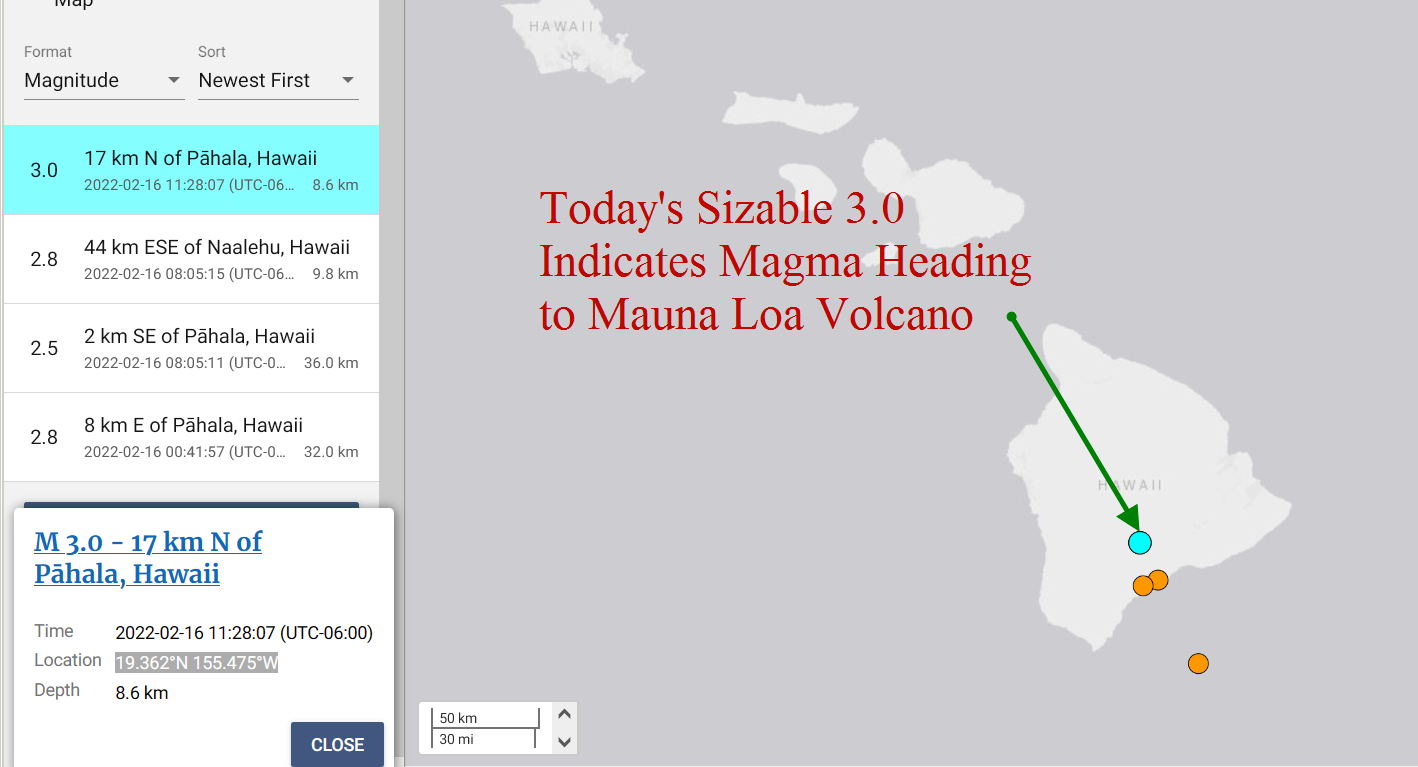
stock here: been watching this closely for many years. Maybe in the 2018 volcanic event there may have been triple 3’s, no time to check, however, this IS very unusual activity.
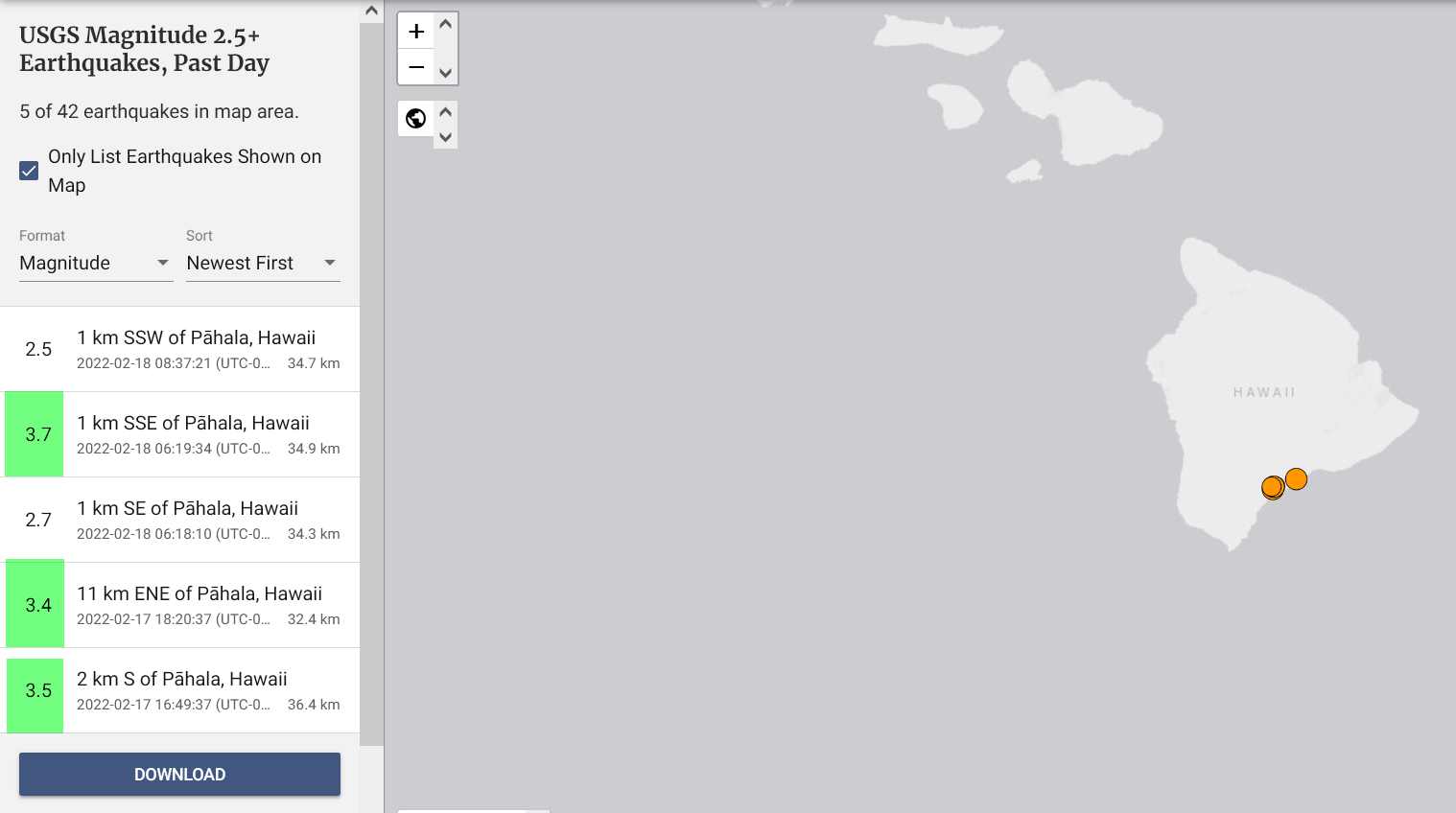
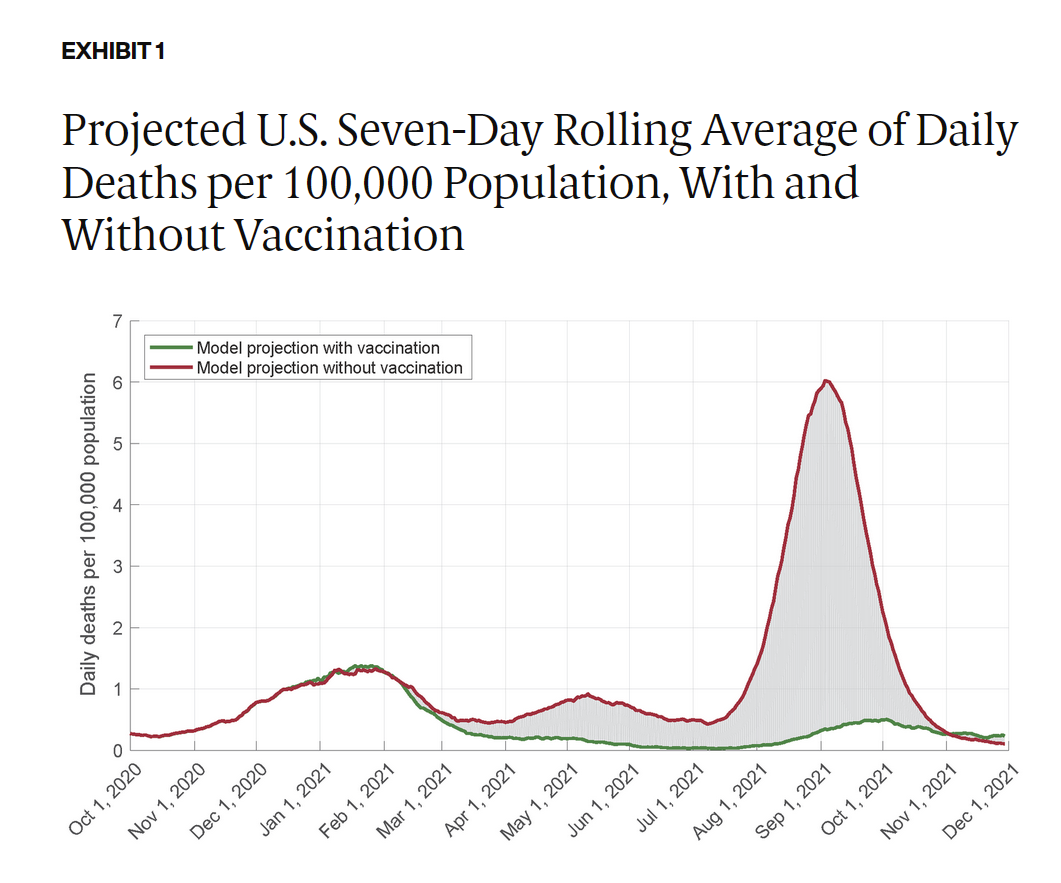
stock here, we all “known” second waves are 5 times worse than the first wave even though R(oe) is much lower because of widespread natural immunity. Shame on them, damn them to hell.
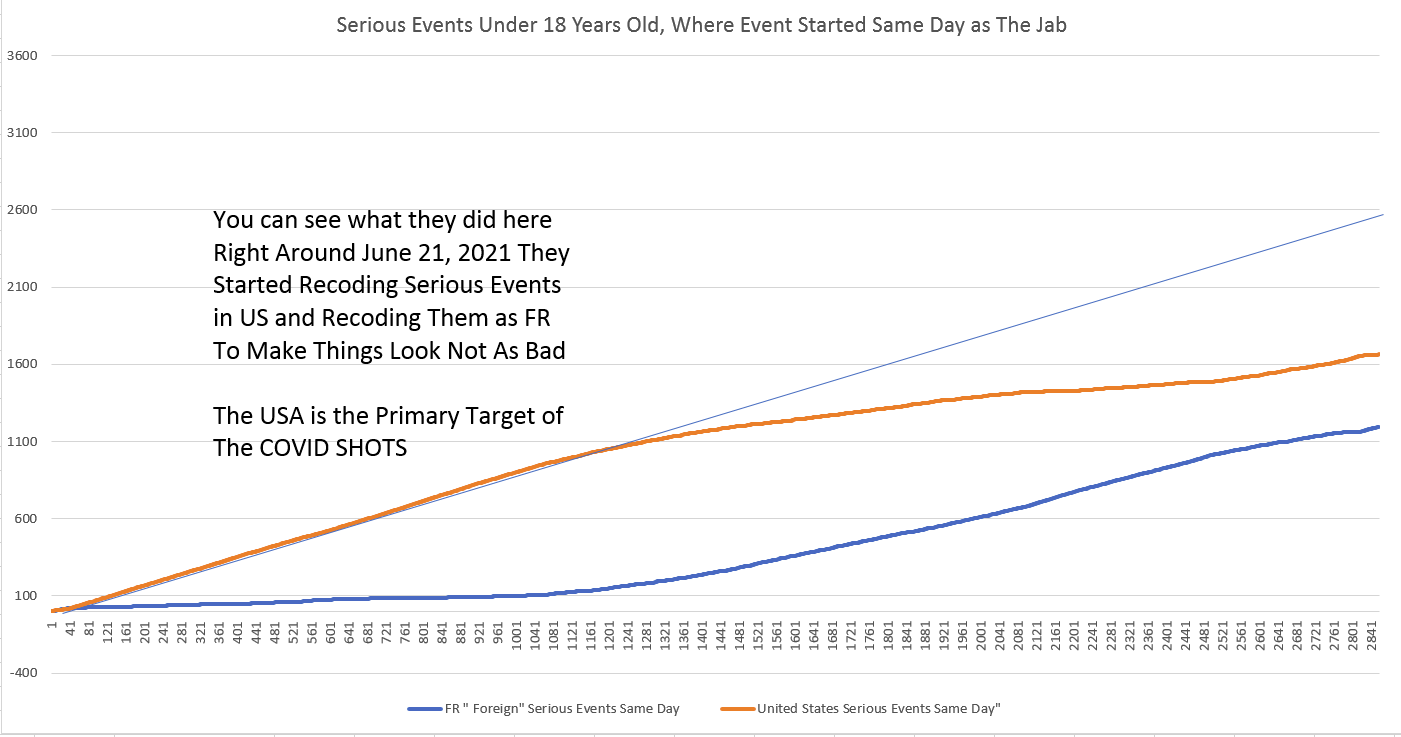
In early June they started a serious campaign of Jabbing those under 15. And the results were not good. Instead of allowing the State of occurrence Code to remain properly in the system, they starting changing the codes to FR “Foreign” aka another country.
I caught them doing the same on the Pregnant Women that they were spontaneously aborting. Of those that aborted, 30% did so on the same day of the jab.
Boom!
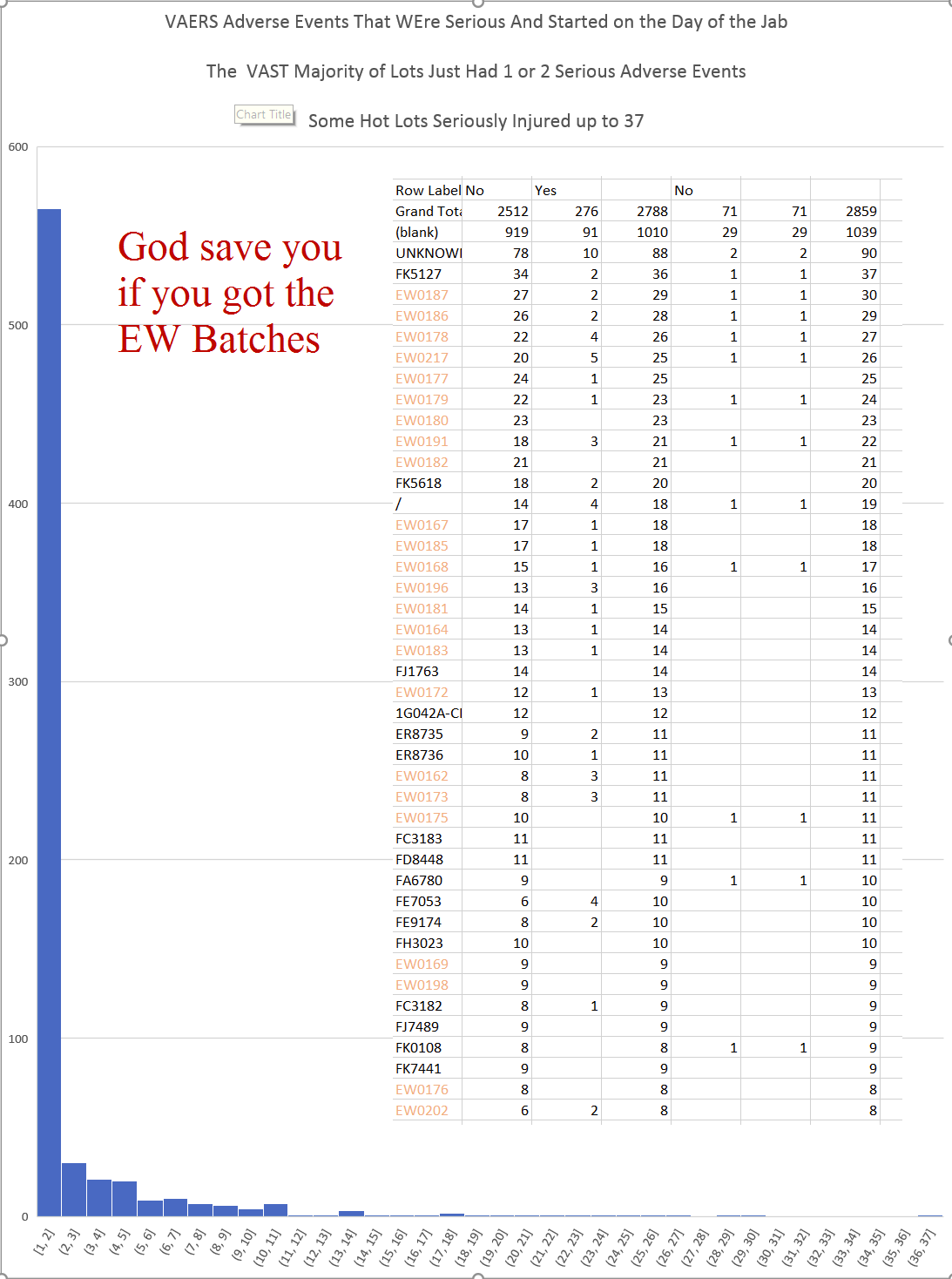
These are “hot lots” that caused serious injury, about 10% of the time, death, on USA under 18 YO…..on the same day of the Covid Shot. Note the histogram, most lots are not Killer Batches. The EW series of batches are horrific.
There is a detailed article a few further down, but here are 2 movies I created using the data. It runs from Jan 1 to Feb 17th, 2022
This first video is from 2021 up to August and shows all of the above sea level earthquakes in time sequence
https://www.bitchute.com/video/YLXuaqtk5d2D/

Today

stock here, you can see my responses below. I thought this poll was a good thing, but it is really Gaslighting and Normalization / Familiarization
https://forms.office.com/pages/responsepage.aspx?id=xt5HOLJj-UOm0FikCqoaEGnYeUiHuopLnLs1JHhRF4RUMVFRSzhUMlRRRlhQVDNSTlBPM044UDBDNS4uIts odd, I cannot embed that link, or post as a link. You will have to copy paste.
Typical strategy of the COVID Great Reset is to dehumanize humans by presenting them as cartoons. Watch how many times that happens now. And note the diversity….Less than 1% of Hawaii is black.
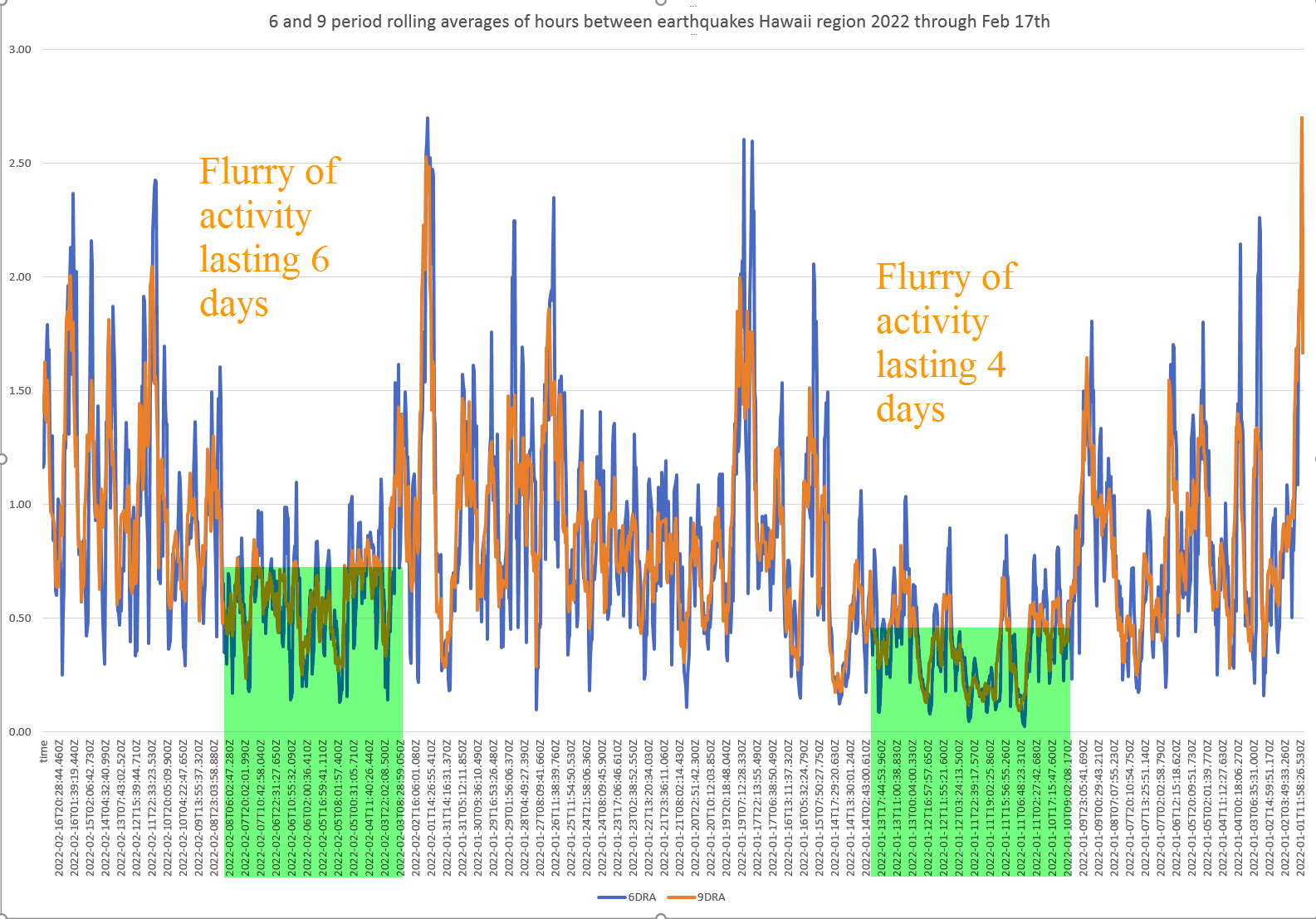
stock here. You never really know what you are going to get when you start with some original research. I have programmed code that automatically creates a chart with days between Earthquakes and then 6 and 9 Rolling Averages on that Data. For Hawaii I switched it to hours between quakes and check the results. I also turned them into 2 movies, maybe you like one of the movie more. 1 shows the huge Maui Earthquake. Drop a comment, what do you think. A look a the two multi-day swarms of earthquakes.
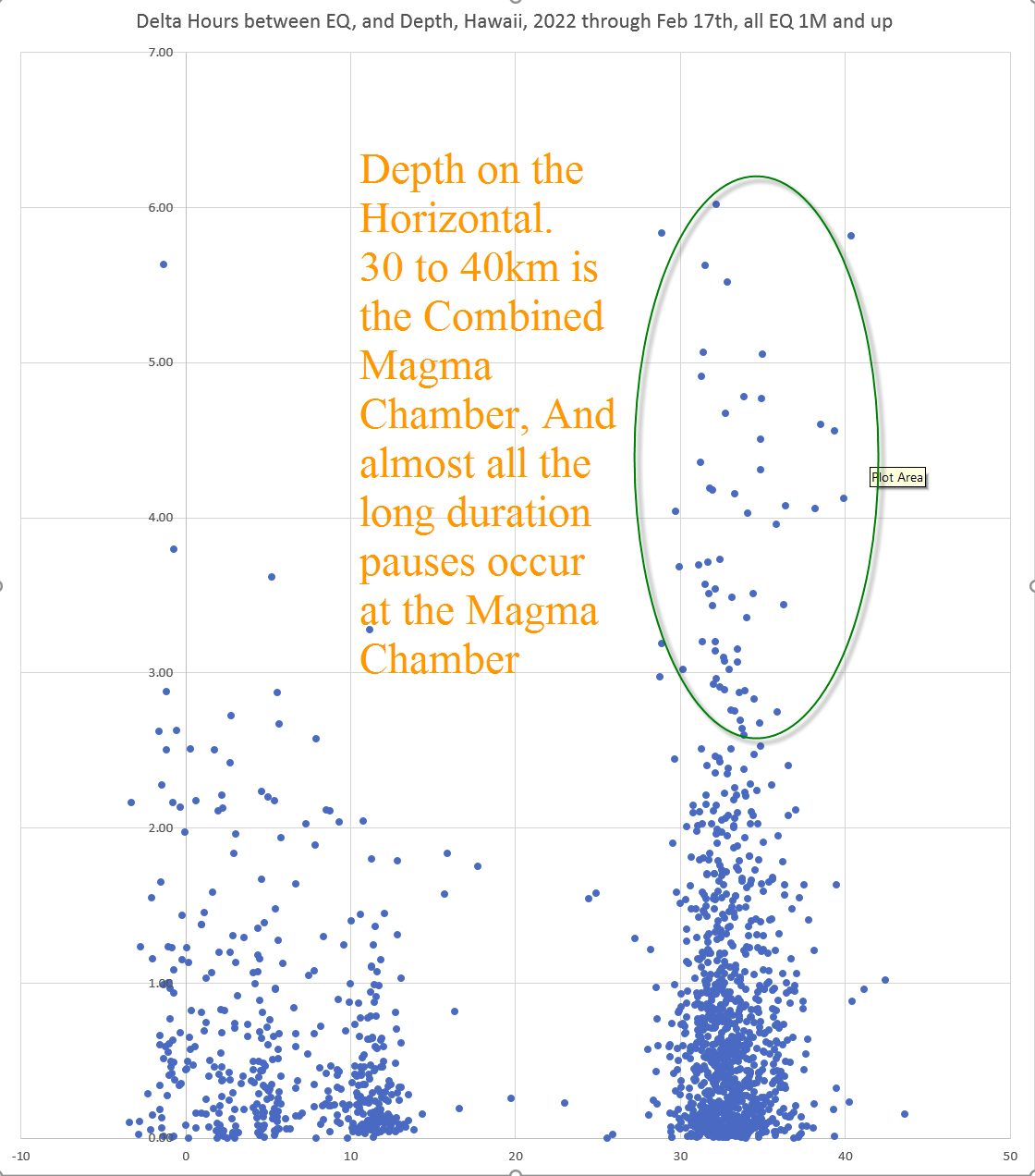
First screencap is from a few days ago. Almost all the Long Duration (4 to 6 hour) lulls occur at the Combined Magma Chamber which the movies will make totally obvious.

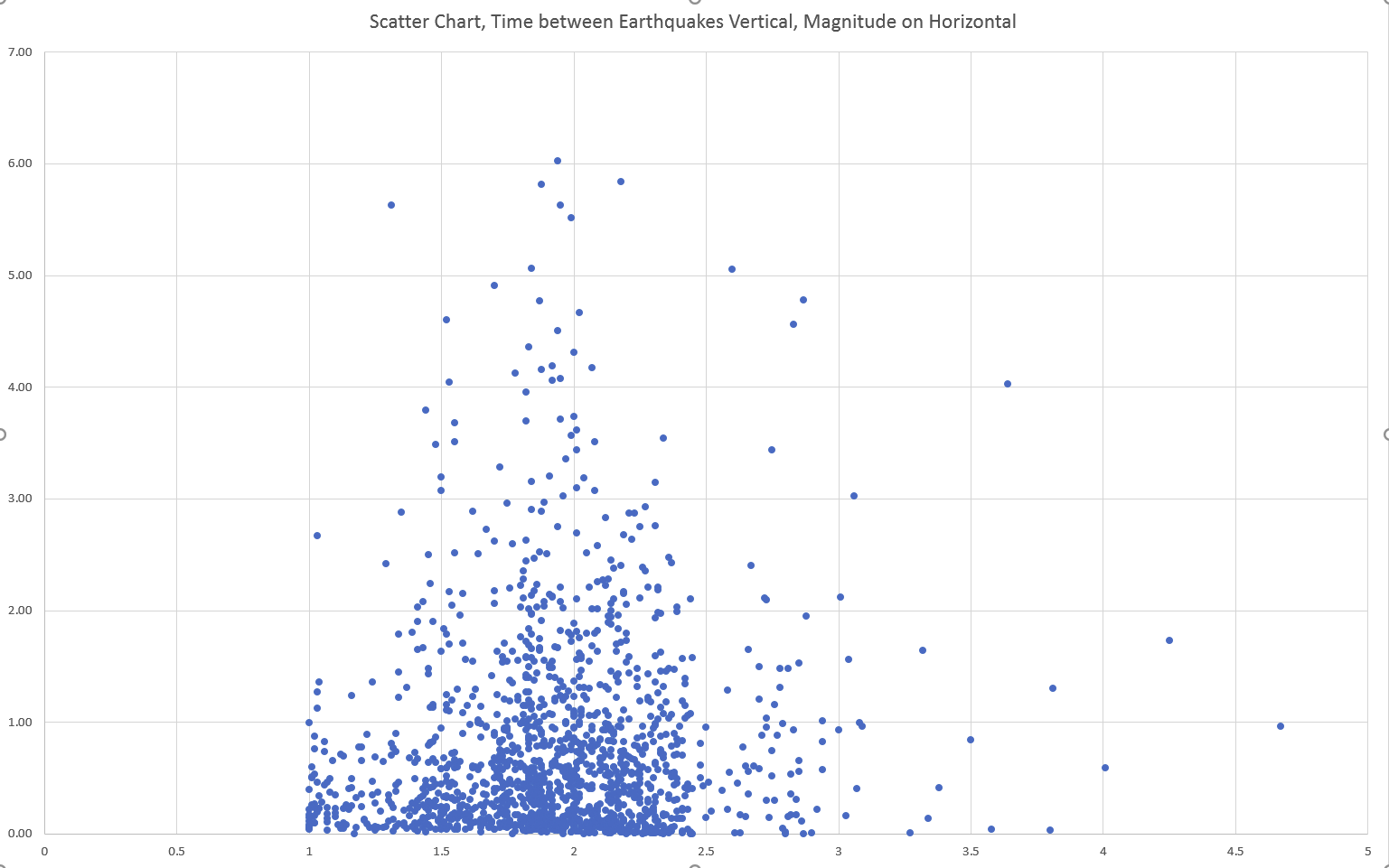
Below is just something I tried, plotting time and magnitude. I don’t really grok any clear lesson from this one, but maybe someone else will spot a pattern. Some large quake aftershock or prior shock analysis could be interesting.
Ottawa city council’s zoom meeting leaked. pic.twitter.com/Y7yIf54bMw
— Citizen 1 (@citizen1448) February 7, 2022#1: They showed up in the Heart of Canadian Darkness, the belly of the beast, the seat of the national government, right in the middle of Ottawa, Canada’s version of DC. The central lesson of the Freedom Convoy is this: truly gain the attention of the elites, we have to go to their house and make them uncomfortable. The formula for success is to make ignoring us – which they would otherwise do if given the option – impossible.
Ottawa City Council: “Our city is under siege… they are terrorizing our residents… torturing them with incessant honking… preventing them from leading their lives… This group is a threat to our democracy.”
#2: Despite the media’s best attempts to smear the participants as “racists,” “terrorists,” etc. (as they always do), the truckers and their supporters come from diverse working-class backgrounds. They are transparently non-violent non-extremists. They’re farmers and truckers of various races – a universally respectable, sympathetic, hard-to-pigeonhole group. Contrasted with the governing class ghouls in opposition to them, they look all the more appealing to the public eye.
The CDC Is “NORMALIZING” Blood Clots Which Are A SIDE EFFECT Of The Covid19 Vaccines:
“Anyone can develop a blood clot!”…..”Even the healthiest athletes!” “Everyone is at risk”.. NO, I’m not as risk because I didnt receive the clot shot…
What a crock of crap. The blood clots are occurring because of the serum in the vaccine which is POISON. But, now, the lying CDC coupled with big pharma got this ALL covered! You’re safe in their hands, eh?
In memory of those who have “died suddenly” from February 1st to 7th, 2022
Once a euphemism for suicide or fatal overdose, “died suddenly” now means exactly what it says—and it’s more common than it’s ever been, worldwide
| Mark Crispin MillerFeb 7 |
We now know, from the statistics, that all-cause mortality has been skyrocketing in countries with the highest COVID “vaccination” rates. Such numbers also tell us that more people all around the world have “died of COVID” than did (reportedly) in all of 2020. (396,837 Americans reportedly “died of COVID” under Trump, while 528,379 have so far “died of COVID” under Biden, whose term started with the US “vaccination” drive.) We also know, from the statistics, that children have been dying in greater numbers since they started getting “vaccinated”—as have professional (and non-professional) athletes the world over, and US military personnel.
Meanwhile, honest witnesses in medicine and the mortuary business, and also first responders, have been telling us they’ve seen a huge increase in sudden and untimely deaths, especially from heart attack, blood clot(s), stroke and cardiac arrest. British undertaker John O’Looney notes an increase of “500 to 600%” in deaths due to thrombosis. Such testimony adds dramatically to our general awareness that this “vaccination” drive is killing people in unprecedented numbers—and clearly by design, or else they would have halted it a year ago, when such grim numbers were already worryingly high.
Such statistics are invaluable; and yet, of course, they’re also too abstract to make us properly aware of the true toll that those “vaccines” are taking on humanity, and in the name of “saving lives.” This is why we need, as much as possible, to demonstrate that countless individuals are dying suddenly and, all too often, prematurely, every day. Only when enough of us have fully recognized this toll will it be possible for us to stop this second, incremental, scattered global Holocaust.
Here are those who have “died suddenly” or “unexpectedly” just this past week, either with no cause given (which is most unusual, even for the elderly), or from a heart attack, blood clot(s), stroke or cardiac arrest, or a very sudden and aggressive cancer (an “adverse event” whose increase has been noted by practitioners like Dr. Ryan Cole).
Bear in mind that most of these are deaths that made the news in one way or another, whereas the vast majority of such surprising deaths go unreported.
Pa. football coach, 40, dies one day after landing ‘dream job’
February 4, 2022
A newly hired high school football coach was supposed to appear for a signing ceremony Wednesday after just landing his dream job. A day later, he was dead.
The tragic story comes from the Pittsburgh Post-Gazette, which reports that Coach Ron Frederick, just hired to lead Southmoreland High School’s varsity football team, died suddenly on Thursday of unknown causes.
Pennsylvania Dunkin’ Employee Dies Suddenly, 16
February 4, 2022
An eastern Pennsylvania community is mourning the loss of a beloved Dunkin’ worker.
Rachel Cox, 16, died suddenly on Jan. 15 at St. Christopher’s Children’s Hospital, according to her obituary. A cause of death was not released.
George Watts Jr., age 24, has died from myocarditis from the Pfizer injection.
February 5, 2022Nashville Angela @AngelasfreenewsGeorge Watts Jr., age 24, has died from myocarditis from the Pfizer injection. The county is currently working on similar cases according to Bradford County Chief Deputy Coroner Timothy Cahill Jr. February 5th 20224,655 Retweets7,050 Likes
We learned this morning that Rachel M. Morgan (VA) died unexpectedly on Wednesday from a sudden illness.
February 4, 2022
The following message was sent to the campus community by Vice President for Student Affairs Ginger Ambler – Ed.
Dear William & Mary Community,
It is with deep sadness that I write to inform you of the death of one of our students. We learned this morning that Rachel M. Morgan died unexpectedly on Wednesday from a sudden illness. Rachel was enrolled in the Mason School of Business’ online MS in Marketing program and was expected to complete her degree in May, 2022.
‘He loved everyone’: Whitestone NY community mourns death of beloved deli co-owner
February 3, 2022
Mario Polito, 44, of Tony’s Beechhurst] Deli, died unexpectedly of a massive heart attack on Saturday, Jan. 29. Polito is survived by his wife, Tania Carucci-Polito, and his 7-year-old daughter, Gianna Marie…
Sheriff’s officials pay tribute to fallen Sgt. Danny Rice
February 4, 2002
Sergeant Danny Rice, with the San Bernardino County Sheriff’s Department, died Wednesday morning after suffering a medical condition, a sheriff’s official said.
In an online video posted Thursday, San Bernardino County Sheriff’s Employees’ Benefit Association President Grant Ward honored Sgt. Rice, who “passed away suddenly after sudden heart failure.”
George Bickham, teacher and mentor to underprivileged children, dies at 46
Bickham worked for 24 years at Perspectives, a supportive housing campus in St. Louis Park.
Jan. 31, 2022
“This guy was truly an angel.”
That’s how Yolanda Farris described George Bickham, who died suddenly in January at age 46.
No cause of death reported.
Jackson community mourns unexpected death of child remembered for style, creativity
January 31, 2022
Wilson’s recollections of Alaya are still vivid and raw as family and friends process her sudden death on Wednesday, Jan. 26.
Alaya had become ill that afternoon, prompting Wilson to pick up his daughter, a seventh grader at Jackson’s Middle School at Parkside, around 1 p.m. that day. He arrived to find her vomiting and complaining of both an upset stomach and migraine headache symptoms.
Wilson dropped Alaya off at her mother Brittney Hamilton’s house, where she continued to try to keep her daughter hydrated and get her to go to sleep. Alaya continued to vomit occasionally, Wilson said, but not to the point they felt they needed to worry about taking her to the hospital.
When Wilson called Hamilton to check on Alaya’s condition around 10 p.m., he got a call back from Hamilton saying Alaya was unresponsive and that she had called 911.
The family is still awaiting results of an autopsy, Wilson said. In speaking with the medical examiner who arrived, there was brown fluid in Alaya’s airway obstructing her breathing, Wilson said.
Wilson said he was not aware of any illnesses Alaya had been experiencing in recent days or weeks, including COVID-19.
Nicaraguan family asks for help with sudden death of brother in Wisconsin
February 3, 2022
PLOVER, Wis. (CBS 58) — A Nicaraguan family in Wisconsin is heartbroken about the sudden death of their brother after a brain tumor was discovered a few weeks ago. Now, they are asking for the community to help in bringing him back home to his homeland to get the funeral and burial he deserves.
Longtime civil rights attorney Davis, 69, dies unexpectedly
February 2, 2022
Phil Davis, a longtime New Mexico attorney referred to as “Mr. Civil Rights of New Mexico” by one colleague, died unexpectedly last week. He was 69.
Maureen Sanders, who graduated from the University of New Mexico School of Law with Davis in the late 1970s and served on an American Civil Liberties Union legal panel with him, said Davis’ death has sent a jolt through the legal community.
“I’m having a hard time talking to you,” she said Tuesday. “It was the loss of a trusted colleague. There are some people in this world you always expect to be there. It was a jolt to me and many others.”
Roswell officer with 23 years of service dies after medical emergency while on duty
February 3, 2022
ROSWELL, Ga. — The Roswell Police Department is mourning the loss of an officer with 23 years of experience on the force after he died unexpectedly on duty following a medical emergency.
The department said in a release Thursday it was “heartbroken” to share the news of Lt. Joel Ruff’s death. They did not detail the exact circumstances of his medical emergency.
Broomfield former chief of police dies unexpectedly
February 3, 2022
BROOMFIELD, Colo. (KDVR) — The Broomfield community is mourning the sudden death of former Chief of Police Tom Deland.
No cause of death reported.
A day after getting dream coaching job, Southmoreland’s Ron Frederick dies unexpectedly
February 3, 2022
Southmoreland High School had its man for a new football coach — and Ron Frederick had the job he always wanted.
Frederick, a 1999 Southmoreland graduate, had interviewed for Southmoreland’s vacant football position Tuesday. On Wednesday, he was informed that he would be the recommended candidate to be hired at a school board meeting next week.
But Frederick died suddenly early Thursday morning of unknown causes.
Beloved North Jersey Mom Of 1-Year-Old Girl Jennifer Lara Dies Suddenly On 33rd Birthday
February 3, 2022
No cause of death reported.
Bob Planthold, giant of disability rights, dies at 73
February 3, 2022
Planthold, a renowned and honored disability, transit and civil rights activist in San Francisco, died suddenly at his apartment on Thursday or Friday of last week. He was 73. The medical examiner has not yet determined a cause of death nor the exact date, Planthold’s sons confirmed, but it was likely a medical episode that triggered a collapse.
Don Lemieux, 65, who coached Olympians and Gardner High to 16 state swim titles, dies
January 29, 2022
Don Lemieux died unexpectedly Saturday. He was 65.
No cause of death reported.
Brian Augustyn, Comic Book Writer and Editor, Dies at 67
February 1, 2022
Brian Augustyn, the longtime comic book writer and editor responsible for bringing writer Mark Waid to The Flash in the 1990s, has died. He was 67 years old. Augustyn passed away after suffering a sudden, severe stroke, according to Waid, who posted the news to Facebook at the request of the Augustyn family.
Harrah Community Mourns As Officer Unexpectedly Dies
January 31, 2022
The Harrah community is mourning the loss of police officer Eric Haskins.
Haskins was a law enforcement officer for more than 15 years in Oklahoma.
He died unexpectedly last week due to an illness.
Some obituary notices from funeral homes, with no details provided. (There are far too many of such notices to track them all and note them here.)
Anthony R. “Tony” Schmeck, 53, of Kutztown, died suddenly on Wednesday, February 2, 2022, in his residence
John A. Regan Jr., 74, of Waukon Iowa died suddenly Monday, January 31, 2022
Isabella Graciela Moscon, age 13, died suddenly, January 30, 2022
February 5, 2022
William Randall “Randy” Parks, of Colorado Springs, CO, died suddenly of medical complications in his home on Wednesday, January 19, 2022
February 4, 2022
Parks was 60.
Robert P. Taylor, Jr., 57, of West Deer Township, died suddenly Wednesday, Feb. 2, 2022, at UPMC Passavant, McCandless
February 5, 2022
Gloria Jean (Gabriele) Dichara, loving mother, grandmother, sister and aunt, died suddenly on January 24, 2022, in Massillon, Ohio
February 5, 2022
Dichara was 79.
David DeLuca, loving husband, father and grandfather died suddenly on Wednesday, January 26, 2022 from complications following heart surgery
February 3, 2022
He was a scholar, musician, photographer, collegiate Hall of Fame athlete, and a well-known Rochester attorney for the past 53 years.
DeLuca was 60.
Mary L. Schropp, 55, of Oxford, died suddenly on Jan. 31, 2022, at University of Iowa Hospitals and Clinics
February 4, 2022
Charles S. Pullara, 91, of Little Falls died suddenly on Wednesday, Feb. 2, 2022
February 4, 2022
Matthew R. Pertrosky, 29, died suddenly Tuesday, Feb. 1, 2022, at his home in Hanover Twp.
Wittman, Grayson Harrison died suddenly at his home in Wittman on Wednesday, January 19, 2022. He was 24 years old
February 5, 2022
Canada
Dalhousie’s ‘Wayne Gretzky of biology’ remembered as ‘most amazing’ human
February 2, 2022
Jeffrey Hutchings, an ecologist and professor at Dalhousie University in Halifax, N.S., was 63 years old when he died unexpectedly Monday.
The cause of death has not been disclosed.
United Kingdom
Brit, 70, dies in ‘happy ending’ massage parlour in Thai party resort Pattaya after panicked masseuse performs CPR
January 28, 2022
Robert John Swain, 70, stripped off his clothes and was lying naked on a massage table while masseuse Miss Oraya rubbed oils into his back when she suddenly realised something was wrong. Mr Swain, who had arrived at the shop on a rented Honda motorcycle this afternoon, started gasping for breath mid-way through the session. Mr Swain was pronounced dead before his body was moved to the hospital. “Everything was going normally then I noticed he was sleeping. Suddenly he started struggling to breathe. He was gasping and choking.
Mystery as two bodies found a day apart in Lanarkshire town as cops launch probes
February 3, 2022
Detectives confirmed that a woman, 30, had died suddenly. And that the death was being treated as unexplained. Worried locals spotted officers on the scene following the grim find.
A spokesperson said: “Police were called around 4.45pm on Tuesday following the sudden death of a 30-year-old woman at an address on Hozier Street, Carluke.
“Enquiries are currently ongoing and the death is being treated as unexplained at this time. The grim find came less than a day before the discovery of a pensioner in nearby Cairneymount Road.
A 65-year-old man was found dead inside the property. Officers also confirmed that this death was being treated as unexplained.
Colchester family devastated after sudden death of young dad, 22
February 1, 2022
A FAMILY is raising money to pay for a funeral after a young dad died suddenly, aged 22.
Blake Wicks, from Colchester, was at his home when he unexpectedly died in the early hours of the morning.
“The paramedics on scene believe it was a heart attack, but they are not sure, and we can’t be certain until the coroner’s report is released to us.”
Devoted dad, 26, who was “life and soul of the party” dies suddenly
February 1, 2022
A heart-broken family is mourning the loss of a devoted dad who was the “life and soul of the party”.
Graham Stephens was home alone on Saturday when his family returned to find he had died, an “unexpected” and “sudden” event which has left the family devastated.
The cause of the 26-year-old’s death is currently unknown.
Brother’s heartbreaking tribute after sudden death of popular Sheffield man, 38, with ‘enormous heart’
February 3, 2022
Tributes have been paid to a “kind and generous” Sheffield man who has died suddenly, leaving friends and family devastated.
Gavin Rodgers, 38, of Parson Cross, was found dead at home early in January but family members are still waiting to hear from the coroner’s office what caused his sudden death.
His younger brother, Josh, of Barnsley, said Gavin’s death was ‘very sudden’ and had been difficult to comprehend for everyone, including his four sisters and two brothers.
Tributes paid to former Argus rugby writer Robin Davey
February 2, 2022
TRIBUTES have been paid to the well-known sports journalist Robin Davey who has died suddenly in his 70s. “Shocked and saddened to hear about the sudden death of Robin Davey former rugby correspondent @southwalesargus passionate about rugby @NewportRFC @dragonsrugby and indeed politics deepest condolences to his wife Sue friends and family,” wrote Matthew Evans, former Newport mayor and leader of the Conservative group on the city’s council. Journalist Tony Poole wrote: “Yes, so sudden + sad. Only last week I was exchanging Twitter banter with him.
Grieving Erdington MP candidate says her dad’s sudden death will drive her on
February 3, 2022
“He was so proud of me – he couldn’t believe I could one day be sitting in the House of Commons.”
Birmingham Erdington’s Labour candidate Paulette Hamilton is speaking of her dad Kenneth Wilson, who died suddenly at the weekend, aged 84, just as her campaign to become the city’s next MP gets in full swing.
PSNI in attendance as man dies suddenly in north Belfast
February 4, 202P2
A man has died “suddenly” in north Belfast on Friday afternoon. A PSNI spokesperson said the man passed away in the Glenrosa Street area of the city.
They said: “Police are currently at the scene of the sudden death of a man in the Glenrosa Street area of Belfast. “There are no further details at this time.”
Sudden death of prominent Northern Ireland businessman, 80
February 1, 2022
One of the last owners of Derry’s Austins of the Diamond department store, Luke Hasson has died suddenly while attending a family celebration in County Louth.
Ireland
Irish school community in shock after sudden death of 34-year-old teacher Emily Seery
February 2, 2022
A school community is in mourning after the sudden death of a young teacher.
Emily Seery, who taught in Coláiste Iosagáin in Portarlington, died suddenly last week to the shock of colleagues and students.
Family left ‘devastated’ following sudden death of young father Odhran Doherty (19)
February 3, 2022
THE family of a caring young father who died suddenly at his home in north Belfast have spoken of how they have been left devastated.
‘He was just a special guy, small in stature but a giant of a man’
February 2, 2022
Best friend pays tribute to the late Bruce Kelliher from Tralee who died suddenly in County Galway this week, aged 48.
The death of Bruce Kelliher at the age of 48 has instilled a deep sense of shock and sadness in Tralee among all who knew him.
Bruce died suddenly near his home in Oranmore, County Galway on Monday where he lived with his wife, Michelle, and sons Ruben, Mason, and Archie.
As well as being a gentleman, Bruce was an exceptional athlete and excelled in basketball, surfing, and skateboarding. These interests ensured that his legion of friends was a vast one as they, and his family, now struggle to come to terms with his death.
Australia
Glenn Wheatley: 74-year-old “double vaccinated” Australia music icon dead after weeks suffering in hospital, mainstream media blame COVID-19
February 1, 2022
It’s unclear when exactly Mr. Wheatley received his injections. But both 7News and the Sydney Morning Herald reported that he was “fully-vaccinated.” An educated guess is that he received the injections in November and/or December last year because reports say he “contracted the virus” around Christmas. He was in the Epworth Hospital intensive care unit “fighting valiantly for several weeks.”.
Greece
Alexandros Lampis dead at 21: Greek footballer dies after cardiac arrest with no defibrillator or ambulance at stadium
February 3, 2022
The shocking incident comes just eight months after Christian Eriksen fell to the turf playing for Denmark at Euro 2020. Like Lampis, the midfielder suffered a cardiac arrest.
Russia
‘Putin Jung’, a doctor in his 50s who gave emergency treatment to Navalni, died suddenly
February 5, 2022
A doctor in his 50s who gave emergency treatment to Alexey Navalni, the ally of President Vladimir Putin, who had been addicted to poison, died suddenly. On the 4th (local time), CNN broadcasts in the United States reported that Dr. Maxmisine Sergei Valentinovich ’suddenly’ died at the age of 55. No specific sign was disclosed. Omsk Emergency Hospital said, “Unfortunately, we are notifying the news that Dr. Maximisin, the deputy chief of anesthesia and resuscitation at Omsk Emergency Hospital No. 1, died suddenly.”
Serbia
Ksenija Vučić, Serbian Journalist and First Wife of Serbian President, Suddenly Dies of Alleged Blood Clot or Heart Failure
January 29, 2022
“Tonight in Belgrade, suddenly at the age of 56, Ksenija Vučić, the mother of our two children, Danilo and Milica, and my first wife, passed away,” Serbian President Aleksandar Vučić announced on his Instagram account.
Estonia
Riigikogu member, volunteer rescue worker, 51, dies
February 3, 2022
Reform Party MP and volunteer rescue worker Madis Milling died suddenly on Wednesday while attending a fire in Saku. Mourning flags are flying on government buildings today in remembrance.
The Rescue Board said Milling, 51, was the first person to arrive at a fire in Saku Municipality on Wednesday night. During the operation, he collapsed suddenly and later passed away.
Norway
Norwegian Cruise Line Crew Member, 36, Dies on Norwegian Escape Following COVID-19 Quarantine
February 1, 2022
A head bartender from India recently died on the Norwegian Escape after he spent ten days of quarantine for COVID-19 on the Norwegian Cruise Line (NCL) cruise ship. The death was first reported by the Crew Center site which is operated by former crew members. The popular site reported that the crew member had been isolated in a cabin on Deck 2 without fresh air and sun for 10 days. A fellow shipmate reportedly stated (a week ago) “yesterday he was out from the quarantine, and this morning Code Alpha was announced on board and he suddenly died.” No cause of death was mentioned.
A family member of the crew member, Sanjip Gurung, recently went to Twitter to request that NCL provide his family with information about his brother’s death after the company’s human resources department repeatedly refused to provide him with information.
(NCL requires all employees, as well as passengers, to be “fully vaccinated” by two weeks prior to departures.)
Subscribe to News from Underground by Mark Crispin Miller
Hundreds of paid subscribers
News from Underground is based on my belief that, like journalists, academics have a civic obligation to help keep the people well-informed, so that American democracy might finally work.

stock here: Its odd to me that the Epoch times does not clearly jump into Bob Sagats death as Vax injured, Vax caused. Basically he dropped to the floor cracking his head, and then crawled into bed because he was in such bad shape he couldn’t even summon help. Then his brain and brain cavity filled up with blood. He had gotten the COVID shot 3 weeks prior.
The this other comedian bragged about being boosted “and Jesus loves me best” and then passes out on stage cracking her skull.
All the evidence points to her fainting being caused by the vaccine.
Did the COVID vaccine cause Heather McDonald to collapse on stage? All the evidence points to her fainting being caused by the vaccine.  Here are the 6 key facts you should know: She was vaccinated 3 weeks ago with a boosterShe has no history of fainting everThe doctors could find NOTHING wrong with her after she went to the hospital (note that they never test for COVID vaccine injury)Her fainting spell was not COVID related. She recently tested negative for COVID.She performed the night before with no incident. She didn’t consume any alcohol before or during Saturday’s showShe was making jokes on stage about being “vaxxed, double vaxxed, boosted” right before she collapsed I believe that the most likely explanation is that the incident was caused by the vaccine. They’ve ruled out every other possible cause. The vaccine is known to cause sudden loss of function and it is most likely to happen within 60 days after the vaccine. In many cases, people simply die instantly with no warning. It was ironic that it happened when she was joking about being vaxxed, wasn’t it? I’m sure none of her doctors will ever consider that the “safe and effective” vaccine caused her collapse. Like Comment Share You’re a free subscriber to Steve Kirsch’s newsletter. For the full experience, become a paid subscriber. Subscribe © 2022 Steve Kirsch Unsubscribe Here are the 6 key facts you should know: She was vaccinated 3 weeks ago with a boosterShe has no history of fainting everThe doctors could find NOTHING wrong with her after she went to the hospital (note that they never test for COVID vaccine injury)Her fainting spell was not COVID related. She recently tested negative for COVID.She performed the night before with no incident. She didn’t consume any alcohol before or during Saturday’s showShe was making jokes on stage about being “vaxxed, double vaxxed, boosted” right before she collapsed I believe that the most likely explanation is that the incident was caused by the vaccine. They’ve ruled out every other possible cause. The vaccine is known to cause sudden loss of function and it is most likely to happen within 60 days after the vaccine. In many cases, people simply die instantly with no warning. It was ironic that it happened when she was joking about being vaxxed, wasn’t it? I’m sure none of her doctors will ever consider that the “safe and effective” vaccine caused her collapse. Like Comment Share You’re a free subscriber to Steve Kirsch’s newsletter. For the full experience, become a paid subscriber. Subscribe © 2022 Steve Kirsch Unsubscribe548 Market Street PMB 72296, San Francisco, CA 94104 |
stock here, just a quick post, stay frosty. Sun is waking up and that will cause EQ and Volcanoes.